AI-Driven Segmentation on Weight Bearing CT Introduction Accurate segmentation is critical for orthopedic workflows, including…
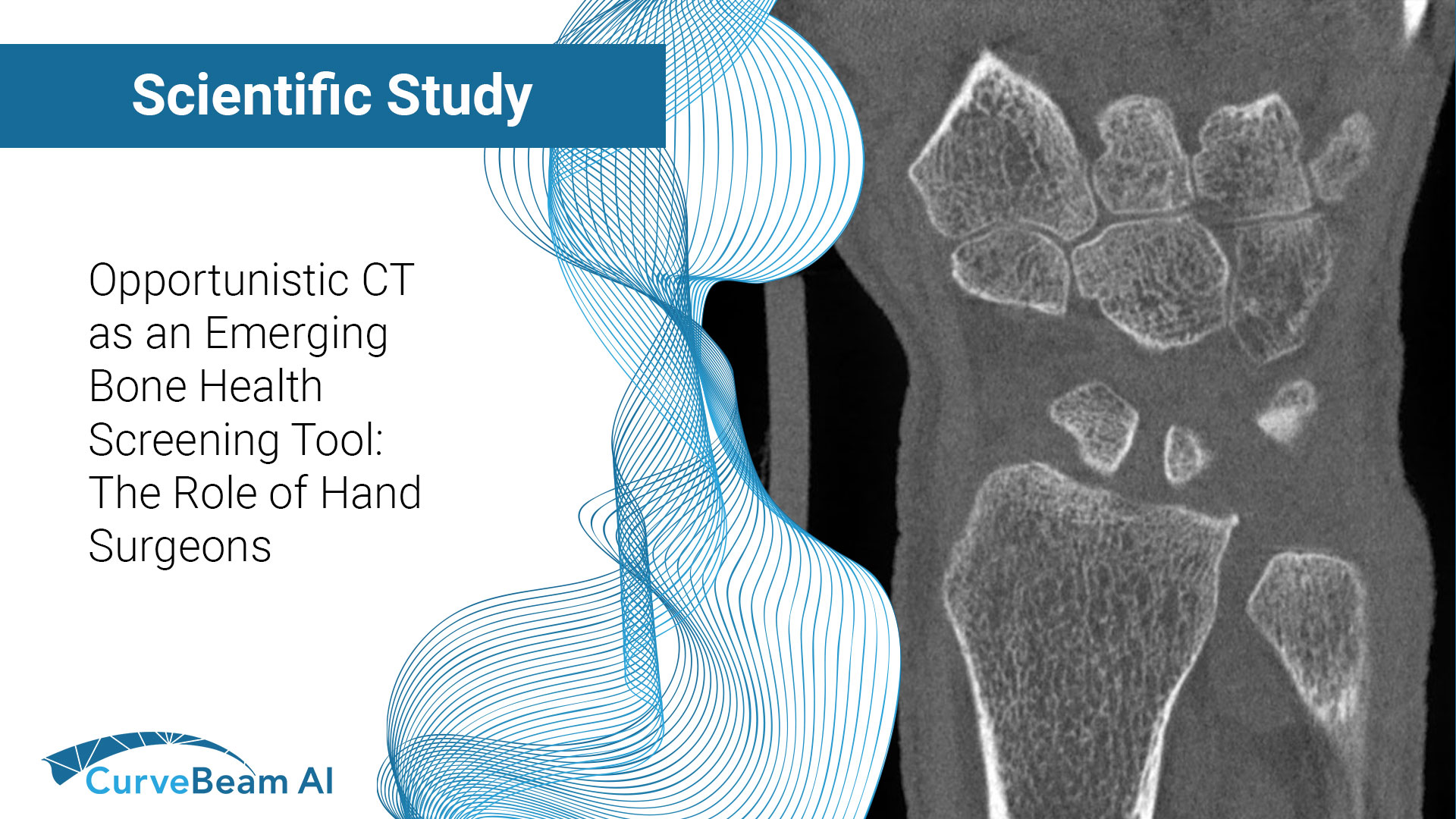
Assessment of Knee Instability in ACL-Injured Knees Using Weight Bearing Computed Tomography
Key Points:
- Anterior tibial translation (ATT) and femorotibial rotation (FTR) are the two most common indicators of an anterior cruciate ligament (ACL) tear.
- The effects of weight bearing have proven to increase the sensitivity to ATT in ACL injured knees and to improve evaluation of femorotibial rotation.
- Researchers have proposed a protocol to quantitatively assess instability in ACL-injured knees using weight Bearing CT (WBCT), after measuring ATT and FTR in various knee positions.
Having patients stand in a 30-degree flexed position bilaterally during a WBCT scan may be adequate for ACL-instability assessment.
Previous studies have reported increased ATT and FTR, measured on medical CT scans, are secondary signs of ACL tears. Increased ATT could be a potential indicator of poor outcomes following ACL reconstruction.
Dr. Renata Vidal Leao et al out of the Hospital Sirio-Libanes, Institute of Radiology in Ovidio Pires de Campos, Sao Paulo, Brazil, aimed to propose a protocol for assessing knee instability in ACL-injured knees using WBCT.
Case Report
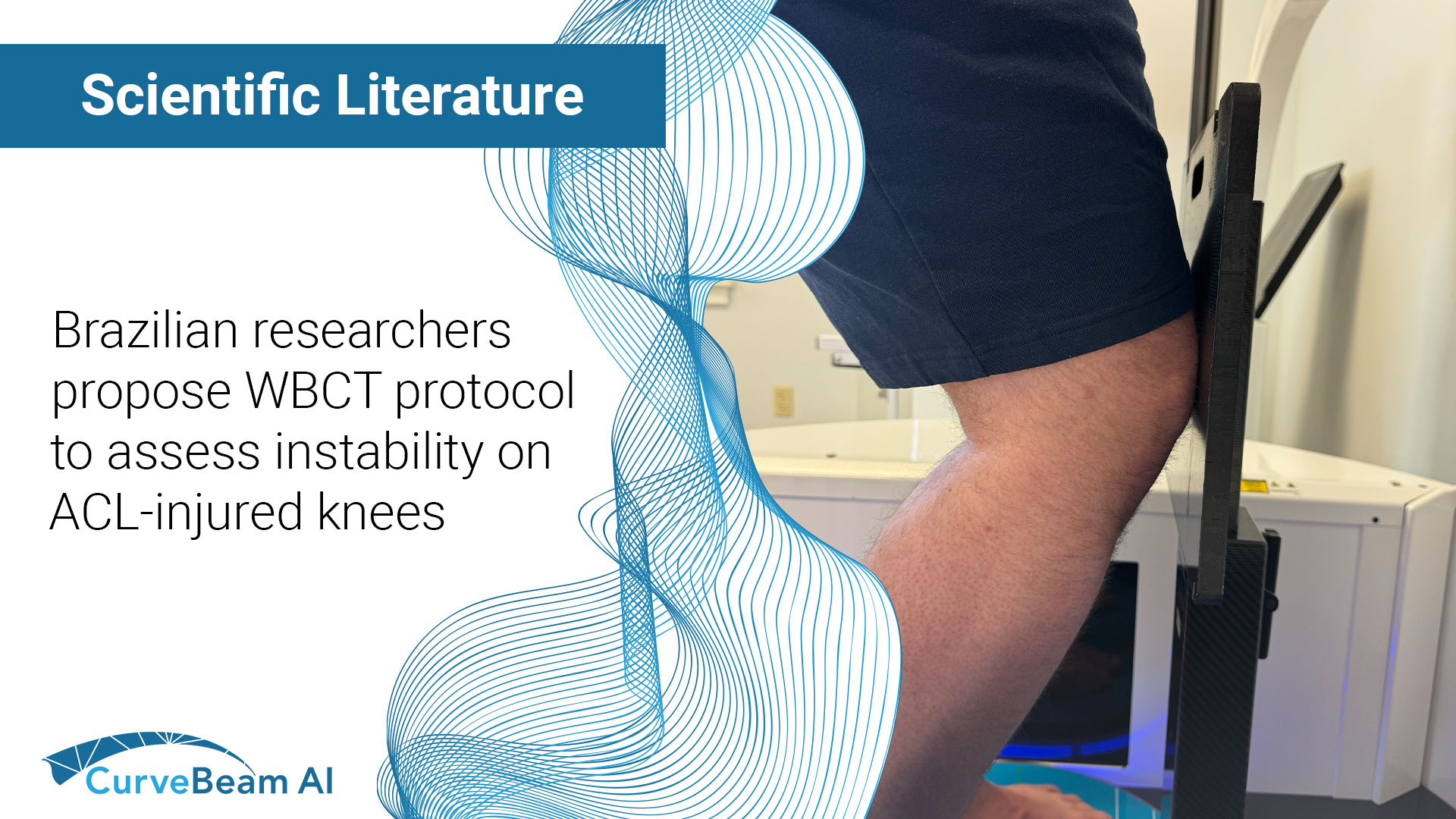
Five patients (male, aged 23-30 years old) with unilateral chronic ACL tears were referred for WBCT scans on a CurveBeam AI LineUP system. Bilateral images were obtained in four positions: (1) bilateral knee extension, (2) bilateral knee flexion, (3) single-leg stance with knee flexion and external rotation, (4) and single-leg stance with knee flexion and internal rotation. Patients were asked to flex 30 degrees for all flexed positions. Patients were asked to distribute weight as evenly as possible in the two bilateral stances. In the single-leg stances, patient were asked to direct weight to the pathalogical leg. Internal and external rotation of 45 degrees was applied to create additional joint stress. Each patient was scanned six times.
The radiation dose, time for protocol acquisition, and patients’ tolerance of the procedure were recorded. A blinded senior radiologist assessed image quality and measured the ATT and FTR angle in the ACL-deficient and contralateral healthy knee.




Patient positioning in WBCT for evaluation of knee instability in ACL-deficient knees. (Left to right) 1. Bilateral extension 2. Bilateral 30 Degree flexion, using a goniometer to ensure adequate flexion degree. 3. Left single-leg stance with knee flexion and internal rotation. 4. Left single-leg stance with knee flexion and external rotation.
Results
The proposed protocol resulted in a 16.2 mGy radiation dose and a 15-minute total acquisition time for the six scans. The procedure was well-tolerated, and patient positioning was uneventful, providing good quality images. In all four positions, mean measurements of medial and lateral ATT were higher in ACL-deficient knees versus the healthy knee. FTR values ranged from 2 to 27 degrees in the ACL-injured knees, versus 0 to 13 degrees in the non-inured knees.
Among all positions, the bilateral knee flexion position showed the highest mean lateral ATT and mean FTR in the ACL-injured knees. The results suggested imaging in a flexed position alone may be adequate.
Conclusion
Researchers concluded that WBCT could emerge as a non-invasive and reproducible method for evaluating anteroposterior and rotatory instability through quantitative measurements.
An unexpected finding was that bilateral flexion had higher mean values for lateral ATT and FTR. Researchers said this could be due to increased muscular stabilization required for the single-leg stance, potentially leading to reduced instability measurements.
To read the full study click here.
Related Posts