Orthopedic decision-making depends on accurate representation of anatomy—particularly when joint alignment and bone relationships change…
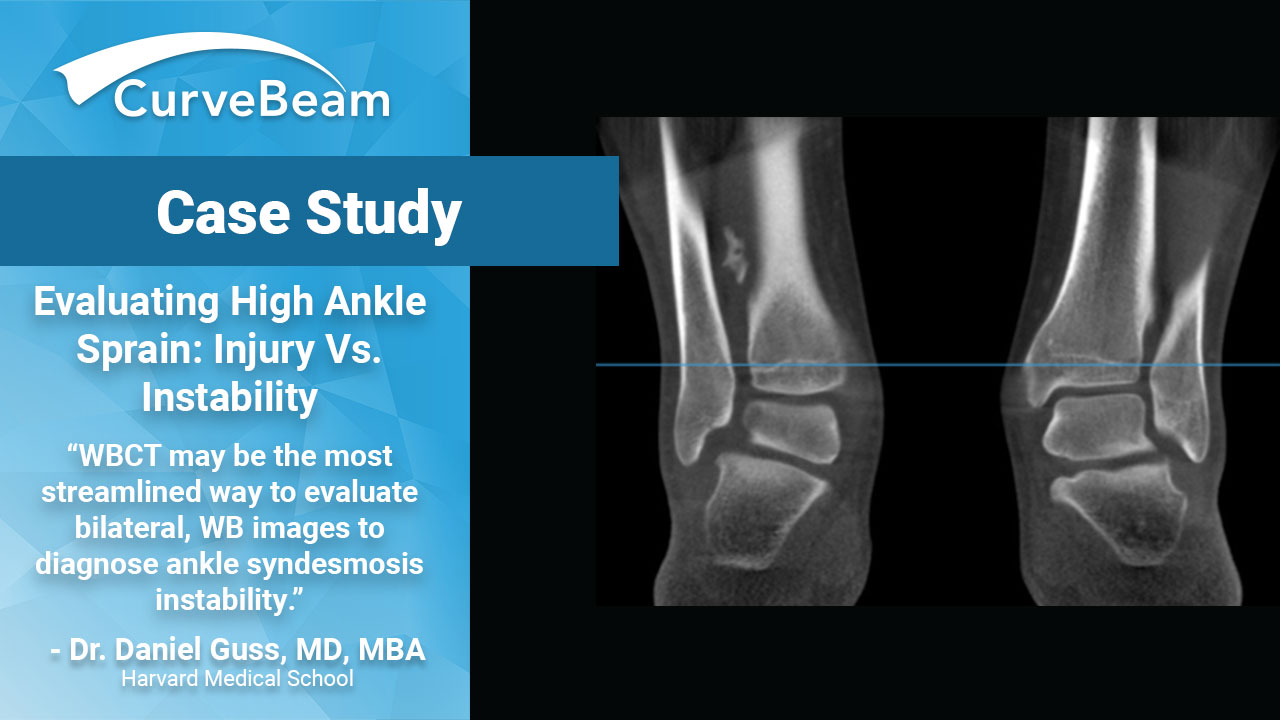
Evaluating High Ankle Sprain: Injury vs. Instability
Syndesmosis – A Functional Injury
Ankle syndesmosis injury, commonly known as high ankle sprain, is one of the most common cases seen by foot and ankle specialists. An estimated 11% of all ankle injuries and 8.5-18% of all ankle fractures have injury to the syndesmosis. An inaccurate diagnosis can lead to chronic problems or repeat surgeries. Common indications for delayed surgery or reoperation include improper diagnosis, malreduction and inadequate fixation.
The syndesmosis connects the tibia and fibula above the ankle joint. One of the most difficult distinctions to make is whether the injury is isolated to the syndesmosis itself or if it has affected the stability of the ankle joint as well.

Dr. Daniel Guss, MD, MBA, assistant professor of orthopedic surgery at Harvard Medical School, took a deeper look at syndesmosis and how weight bearing CT imaging could improve diagnostic ability in a presentation he delivered to the WBCT International Study Group in July 2018.
Syndesmosis – Variabilities Are Common
The ankle syndesmosis serves two main functional purposes. First, it is designed to maintain the spatial relationship between the tibia and fibula in order to stabilize the ankle mortise throughout weight bearing activity. Second, it allows for flexibility of the ankle mortise in the coronal plane along the talar dome throughout various degrees and dorsiflexion and plantarflexion.
Dr. Guss reminded clinicians that when assessing the functional ability of the syndesmosis, it is important to note that recent studies have shown considerable variability in the concavity of the incisura, bony overlap, and clear space within the ankle mortise from one patient to another. In this regard, comparative anatomy images of the left and right ankle are essential for a thorough evaluation.
Clinical Exam
During a physical exam, the most common tests for evaluation of syndesmosis injury are external rotation stress test, calf squeeze test, and cross-legged test. By and large, all of these tests give greater indication of injury, but all have low sensitivity and specificity, Dr. Guss said. In addition, a positive test from any of these maneuvers is not considered diagnostic.
Imaging – Need for Contralateral Evaluation
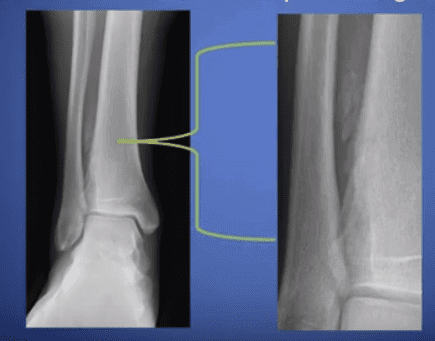
Once history and physical exam have been completed, most clinicians turn to initial standard radiographs for evaluation. Tibia/fibula overlap, tibia/fibular clear space, and medial clear space are most often the areas of focus for more definitive diagnostic information in regard to instability. Most will attempt dynamic stress radiographs with high level of clinical suspicion.
However, Dr. Daniel Guss explained the importance of contralateral evaluation, as there has been great variability in measurements of the syndesmosis using weight bearing CT imaging within the same joint when measured in neutral, maximum external rotation, and maximum internal rotation. There is also evidence of significant syndesmosis measurement difference in weight bearing versus non-weight bearing images of uninjured ankles. This further illustrates the flexibility of the syndesmosis as a support structure.
Finally, if MRI is believed to be necessary, it is important to remember that this modality is very successful at detecting injury, but it does not shed any light on instability as it is a non-weight bearing image, Dr. Guss said.
Case Study – Undetected on X-Ray
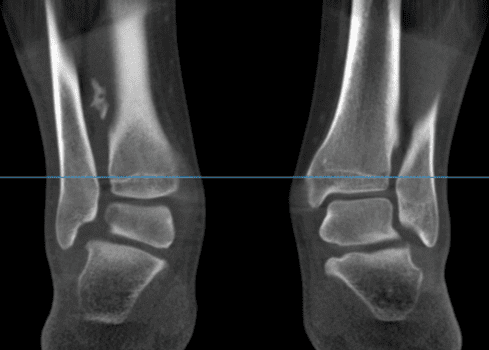
Dr. Guss shared a case in which a 20-year-old male fell down a flight of stairs and thought he had sprained his ankle. He went to his college health services and obtained an X-Ray, which was negative for fracture. However, the X-Ray did show subtle calcifications within the syndesmoses.
X-Rays taken four months later at Dr. Guss’s clinic showed heterotopic ossification in the syndesmotic region.

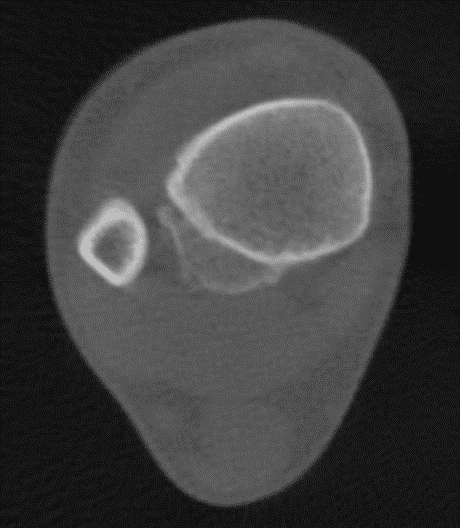
Dr. Guss ordered a pedCAT weight bearing CT so he could assess the HO further. He was able to see the asymmetry under physiologic load at the distal tibio-fibular articulation and also that the HO was forming posterio-laterally.
The patient ultimately underwent an excision of the HO and fixation.
Case Study – Subtle Asymmetry
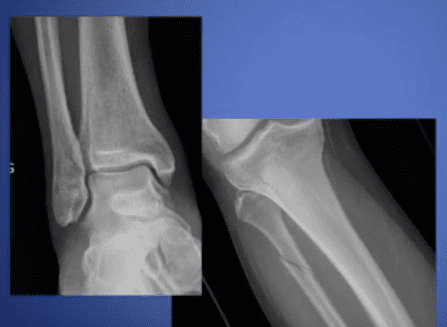
Dr. Guss shared another case where a Gentleman in his 50’s presented to the ER complaining of right ankle and lower leg pain after slipping on ice. Traditional x-rays were obtained, and he was diagnosed with a Maisonneuve-type injury with proximal fibula fracture and medial ankle sprain.
Upon follow up, the patient had a weight bearing CT scan done of both ankles that allowed for cross-section comparison under physiologic stress. This scan revealed subtle asymmetry and widening between the distal tibia and fibula of the injured right ankle compared to the non-injured left ankle.
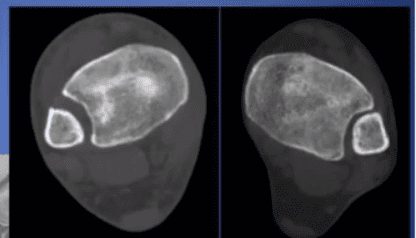
Subsequently, this patient went on to have surgical fixation performed despite being told originally that he had simply sprained his ankle.
Key Take-Aways
In conclusion, syndesmosis injury can be easily missed and yet carries long term implications for functional instability and chronic pain. When considering what imaging studies are necessary, it is essential to look at weight bearing and contralateral images to obtain a thorough picture of functional anatomy specific to that patient. As weight bearing CT technology becomes more widely available, this may be the most streamlined way to evaluate bilateral, weight bearing images to diagnose ankle syndesmosis instability.
Watch Dr. Guss’ entire lecture here:
Related Posts