AI-Driven Segmentation on Weight Bearing CT Introduction Accurate segmentation is critical for orthopedic workflows, including…
Visualizing TFCC Tears at the Point-of-Care

Ritesh Durgapersad, RT(R) ARMIT
The triangular fibrocartilage complex (TFCC) is a major stabilizer of the distal radioulnar joint. An injury to the triangular fibrocartilage complex can result in chronic wrist pain. TFCC tears can be difficult to diagnose via imaging as it is an intrinsic small and thin structure with complex anatomy(1) .
Current Standard of Care
Magnetic resonance imaging (MRI) can provide precise visualization of these structures. A 3 Tesla MRI scan is the current standard of care to acquire high spatial, high contrast imaging data of the intrinsic small and thin structures of the TFCC. Patients are typically put in the “superman position” with the hand raised up and above the head.
Value Proposition CBCT Arthrogram
Cone beam CT arthrogram (CBCTa) may be useful for assessment of the TFCC. CBCTa may be a more comfortable and cost-effective alternative that could be utilized at the point-of-care.
Potential advantages over traditional MRI scan include:
- Patients do not need to schedule with or travel to an outside facility for an MRI exam.
- Treating physicians can know as soon as the patient’s first visit if there is a TFCC tear; there is no delay in devising a treatment plan.
- Patient with metal implants, who would be restricted from MRI exam, can obtain advanced diagnostic imaging.
- Digitally reconstructed radiographs are presented with every scan, eliminating the need for a preliminary X-Ray.
- Surgeons can review the full high-resolution scan in conjunction with the radiology report for optimal pre-surgical planning.
Potential positioning advantages include:
- Patients do not need to extend their hand upward into superman position.
- The scan is performed in 25 seconds, as opposed to 45 minutes for an MRI exam.
- A patient is injected with 1cc or less of contrast, as opposed to 8-10cc required for an MRI exam.
Financial advantages include:
- A CT arthrogram of the wrist is reimbursed via is CPT code 73201* (CT upper extremity w/contrast.) The 2022 Medicare national payment amount for 73201 is $237.81.
- A CT arthrogram could also be reimbursed via CPT Code 76377* (3D Rendering with Interpretation). The 2022 Medicare national payment amount for 76377 is $80.91.

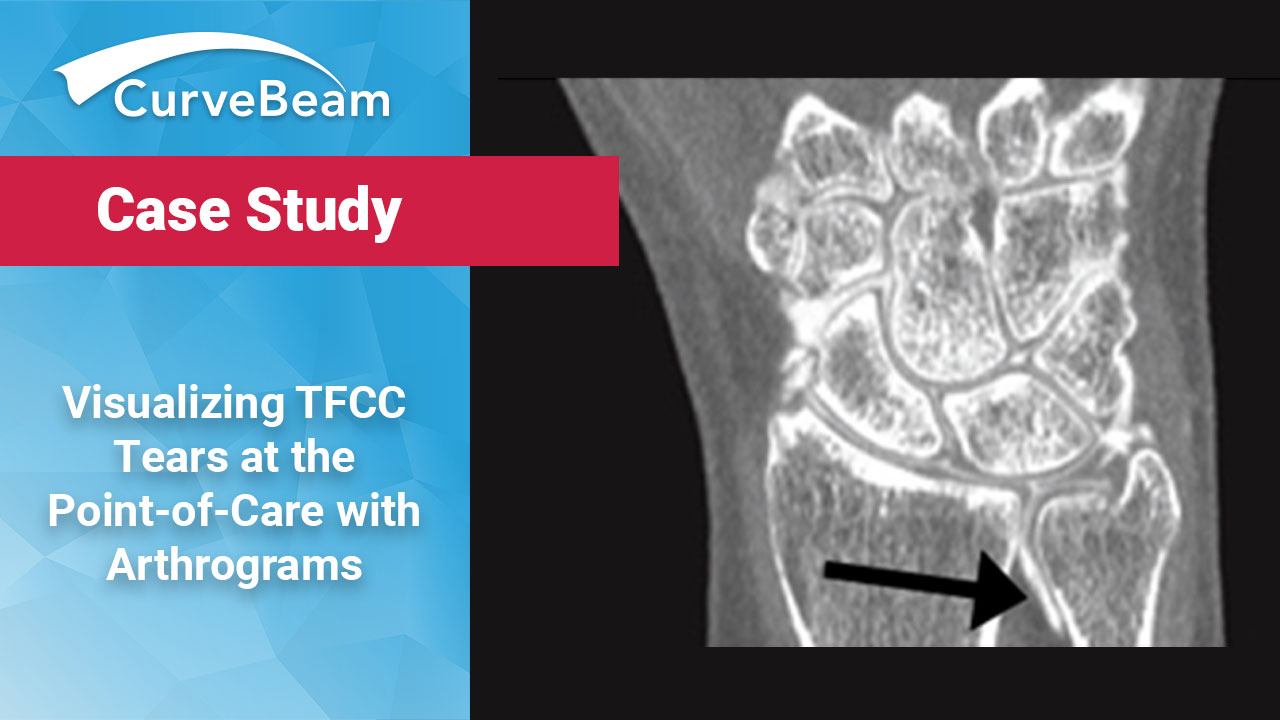
A female patient her mid-40s presented with wrist pain. The CT showed a free edge tear along the radial attachment.
Technique for Cone Beam CT Arthrogram
The treating physician injected 1cc of iodine contrast mixed with 3cc of steroid and 0.5cc of lidocaine. The injection approach was directly into the mid carpal space. The physician used fluoroscopy to guide the needle correctly. After injection of the contrast, the technologist instructed the patient to flex her wrist back and forth, and then performed a CT exam of her wrist. The patient was positioned in a normal seated position and placed her wrist inside the InReach bore. The scan was performed in 25 seconds. No recovery time was required after scanning.

The treating physician ordered an InReach exam as the first line of imaging. (Left) Small osseous bodies adjacent to the ulnar styloid were suspected. (Right) A small pinhole tear was identified along the radius of the triangular fibrocartilage.
The treating physician ordered an InReach exam as the first line of imaging. (Left) Small osseous bodies adjacent to the ulnar styloid were suspected. (Right) A small pinhole tear was identified along the radius of the triangular fibrocartilage.
The InReach provides 0.25mm axial, sagittal and coronal reformats (MPRs). The interpreting radiologist reported no acute cortical fractures, but small osseous bodies adjacent to the ulnar styloid were suspected. A small pinhole tear was identified along the radius of the triangular fibrocartilage.
The interpreting radiologist found the carpal bones to be in normal alignment and the scapholunate ligament intact. However, there was a communicating tear of the lunotriquetral ligament with no diastasis.
(1) Ng, A., Griffith, J. F., Fung, C., Lee, R., Tong, C., Wong, C., Tse, W. L., & Ho, P. C. (2017). MR imaging of the traumatic triangular fibrocartilaginous complex tear. Quantitative imaging in medicine and surgery, 7(4), 443–460. https://doi.org/10.21037/qims.2017.07.01
*These guidelines are intended to outline the basis for coverage and reimbursement for certain imaging services to the extent the services may be covered by a particular payor. They do not in any way guarantee actual payment and are not intended as legal advice. Healthcare providers should exercise clinical judgement when selecting codes and submitting claims to accurately reflect the services rendered. Further, proper coding may require analysis of statutes, regulations or payor contracts and policies, and as a result, the proper code result may vary from one payor to another. It is the provider’s responsibility to determine and submit appropriate codes, modifiers and charges for the services that are rendered. For appropriate code selection, you should contact your local payor prior to submitting claims.
Related Posts